Public Health England investigation report into outbreak of norovirus at Splashes leisure centre, Rainham
11:00, 11 May 2017





Public Health England's report following their investigation into an outbreak of norovirus at Splashes leisure centre, Rainham in October 2016.
Note: appendices referred to in the report were not made available to KentOnline.
1. Notification
1.1. On Monday 31st Oct 2016, the Kent Health Protection Team (HPT) of Public Health England South East was contacted by the management of Thames View Primary School regarding a suspected outbreak of gastrointestinal illness among 16 pupils. The school management suggested that the illness might have been linked to pupils attending the swimming pool at Splashes leisure centre in Rainham.
1.2. On the same day, PHE Communications team were also contacted for a statement regarding the incident. There were reports in the national media that children had fallen ill after swimming at Splashes pool the previous week. It then became apparent that there had been concerns raised on social media over the preceding weekend.
2. Initial actions
2.1. Working with Medway Council Environmental Health Department (EHD) – PHE South East contacted Medway Council Environmental Health Officers (EHOs) to notify them of the incident, to gather additional information and to coordinate investigations. Medway Council’s EHOs reported to PHE that Medway Council had also received a number of complaints directly from pool users and that the majority of ill people had attended a Halloween party at the pool on 28th Oct 2016.
2.2. Infection control measures – PHE provided the school management advice on exclusion and health advice for ill pupils. Medway Council EHOs confirmed that the pool management had already implemented a range of control measures, including super-chlorinating the pool on Saturday 29th Oct 2016 and on Monday 31st Oct 2016 and deep-cleaning of the toilets, changing rooms and other communal areas.
2.3. Public health response - In line with standard procedures, PHE South East took the lead in investigating the outbreak, with the support of other relevant stakeholder organisations.
2.4. Communications - PHE communications and Medway Council communications teams liaised closely to provide updates on the investigations and to respond to media enquiries.
3. Setting
3.1. Splashes leisure centre is a popular facility among families and includes a fun pool with wave machine and flume.
3.2. The swimming pool facilities are especially popular among families with young children during school holidays.
3.3. The main pool, toddler pool and flume are linked to a common water system with an automatic chlorine dosing and filtration system. Regular maintenance and monitoring of the pool water safety is done by staff of the facility, in line with written policies and protocols.
3.4. As part of Halloween celebrations, a pool party was held between 6 and 8pm on Friday 28th Oct 2016. A red dye was added to the pool water system to give the appearance of blood.
4. Incident management
4.1. PHE South East led the outbreak investigations and management, supported by other key stakeholders such as Medway Council EHD, Splashes pool management and PHE Field Epidemiology Services (FES).
4.2. The leisure facility is owned and operated by Medway Council and regulated by the Health and Safety Executive (HSE).
4.3. It is important to note that PHE did not undertake a full review of pool maintenance procedures at Splashes leisure centre. PHE sought and received information from pool management regarding maintenance procedures linked to the outbreak.
4.4. PHE and Medway Council EHD notified HSE of the outbreak and kept them updated on investigations and management.
5. Investigations
5.1. Epidemiological
5.1.1. A retrospective cohort study was undertaken to capture information on pool users between 26th and 28th Oct 2016.
5.1.2. An electronic survey questionnaire (Appendix 1) was prepared and piloted by PHE staff and communicated on 10th November 2016 through a number of routes to pool users:
- by postal letters to those who complained to Medway Council
- by postal letters to those who submitted a stool sample
- by posting a news item on the Medway Council website with direct link to the survey site
- and finally, a cascade through the social media page set up by users affected by the outbreak
5.1.3. The survey closed 27th Nov 2016. A member of public requested access to the survey on 28th Nov 2016 hence it was reopened until 2nd Dec 2016 to allow questionnaire completion.
5.1.4. Cases were defined as individuals who visited the pool facility between 26th and 28th Oct 2016 and developed symptoms of diarrhoea and/or vomiting in the six to 72 hours after their visit to the swimming pool.
5.1.5. Descriptive and statistical analysis was undertaken to identify factors associated with illness.
5.2. Microbiological
5.2.1. Stool samples were requested by Medway Council EHOs from twelve symptomatic cases who reported visiting Splashes pool. Samples were referred to the PHE collaborating laboratory in Brighton to test for the presence of bacterial and viral pathogens.
5.3. Environmental
5.3.1. PHE and Medway Council EHOs investigated pool maintenance procedures and obtained detailed information from the pool management on actions undertaken prior to and following the outbreak.
5.3.2. Results of water sampling tests undertaken by the pool management were shared with PHE.
5.3.3. By the time the incident was notified to public health authorities on 31st Oct 2016, the pool management had already implemented super-chlorination of the pool (twice) and deep-cleaning of all communal areas. Therefore, additional environmental testing would not have contributed useful information in the investigation and management of the outbreak.
6. Results
6.1. Epidemiological
6.1.1. Due to ICT failure at the pool facility, the number of visitors to the pool between 26th and 28th Oct 2016 had not been recorded therefore an overall response rate could not be determined. The leisure manager estimated that approximately 340 people used the pool facilities on 28th Oct 2016, of which 140 had attended the Halloween party.
6.1.2. A total of 96 questionnaire responses were received, of which 93 responses were included in the analysis. Three duplicate responses were discarded.
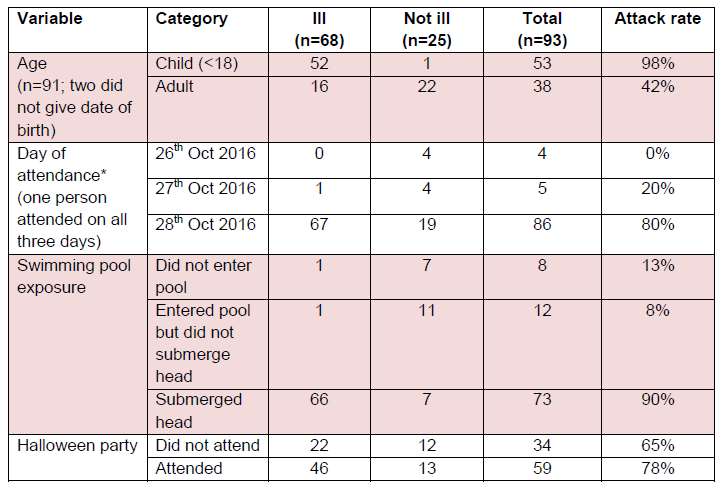
6.1.3. Among the 93 respondents, 68 (73%) met the outbreak case definition. The key characteristics of survey respondents are shown in Table 1.
6.1.4. The most frequently reported symptoms were vomiting (96%), cramps (93%) and nausea (79%). The median duration of illness was three days (range: one to more than five days).
6.1.5. The median age of respondents was 12 years (range 0 to 57 years).
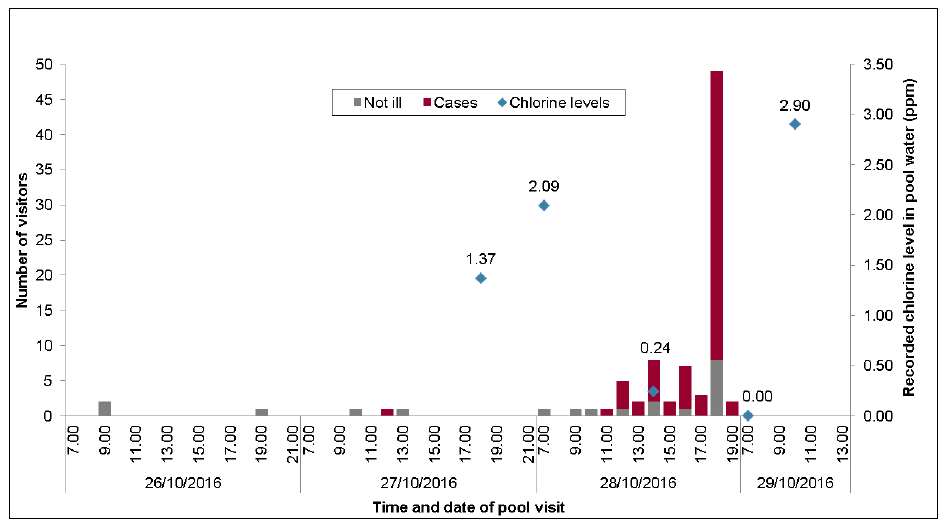
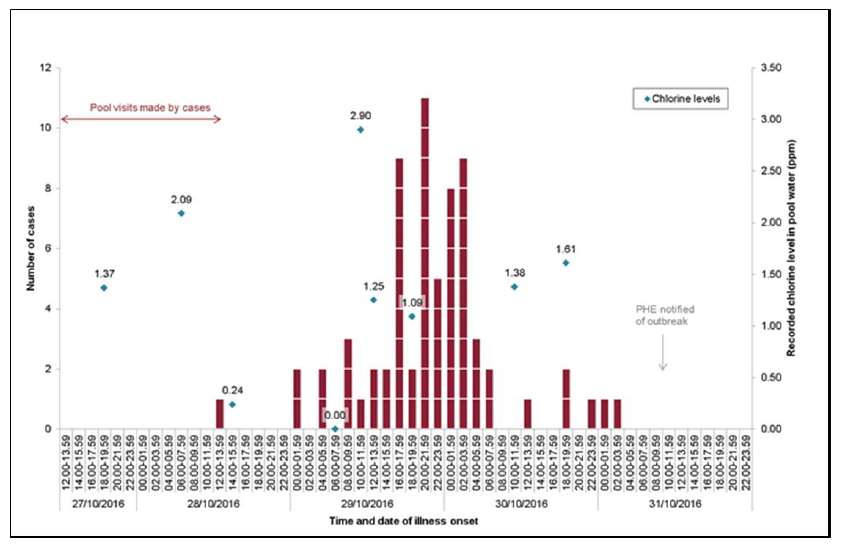
6.1.6. The median incubation period was 28 hours (range 6 to 56 hours).The timing of pool visit amongst cases ranged from 12.00 on 27th Oct to 19.00 on 28th Oct 2016 (Figure 1). Symptom onset peaked 24 hours after the end of the Halloween party (Figure 2), consistent with a point-source outbreak.
6.1.7. Fourteen people reported that they sought medical advice from their GP, A&E or NHS 111. Two reported that they were admitted to hospital.
6.1.8. Ninety percent of cases reported missing at least one day of work or school. In total, cases reported missing 125 days of work or school as a result of their illness.
6.1.9. Among all respondents, one adult reporting becoming ill despite not entering the pool water.
6.1.10. The majority of respondents attended the pool on 28th Oct 2016 (Figure 1). Fifty-nine respondents reported attending the Halloween party on 28th Oct 2016. This constitutes an estimated survey response rate of 42% (59/140) for Halloween party attendees. The attack rate amongst survey respondents who attended Halloween party was 78% (46/59).
6.1.11. Among the survey respondents, 19% (18/93) reported using the shower prior to entering the pool. Sixty percent (56/ 93) reported showering after the use of pool.
6.1.12. In the univariate analysis, entering the pool after the chlorination system was turned off at 1200hrs on 28th Oct 2016 was associated with a 41-fold increase in the odds of being a case (OR 41, 95% CI 4-369; p <0.0001) compared to not entering the pool. Similarly, compared to not entering the pool, submerging head in water and swallowing water were associated with a 66-fold (OR 66, 95% CI 7-617; p<0.0001) and 206-fold (OR 206, 95% CI 16-2579; p<0.0001) increased odds of becoming a case, respectively. There was also good evidence that using any changing room (OR 26, 95% CI 2-1190; p<0.001), entering the swimming pool on 28th Oct 2016 (OR 26, 95% CI 2-1190; p<0.001) and visiting the pool on Friday 28th Oct 2016 (OR 21, 95% CI 2-986; p=0.01) were associated with an increased odds of becoming a case.
6.1.13. Based on the results of univariate analysis, five swimming pool exposures were included in the multivariate model; changing room use, Halloween party attendance, pool entry time in relation to turning off of chlorination system, submerging head under water and swallowing pool water. The model was based on 91 observations, as there was missing age information for two of the respondents. Submersion of head in the pool was associated with a five-fold increase in the risk of being a case compared to not entering the pool (OR 5.5, CI 0.002-13097; p=0.0001).
6.1.14. Additional information on the cohort study findings can be found in Appendix 2.
6.1.15. Some respondents provided free text comments in the survey questionnaire. None of the respondents reported witnessing anyone being unwell whilst at the pool. Some respondents that there were faeces on the floor/toilet seats and nappy bins were broken, necessitating them being opened by hand. Other comments included respondents noticing ‘bits floating in the pool’ and the pool water appearing murkier than usual. One respondent who visited early in the morning reported than the changing room facilities had appeared clean.
6.2. Microbiological
6.2.1. Twelve stool samples were tested at the Brighton laboratory. Of these, eleven samples tested positive for norovirus genotype 2, and were negative for other standard bacterial and viral pathogens. One sample was negative for all standard bacterial and viral pathogens including norovirus.
6.3. Environmental
6.3.1. The swimming pool maintenance and operations at Splashes are underpinned by Medway Council’s Swimming pool Normal Operating Procedure (NOP), Issue 3, dated Sept 2015 (Appendix 3).
6.3.2. An automatic dosing system was in operation, which constantly monitored the free chlorine level and administered doses accordingly. The leisure manager reported that the unit was functioning correctly in late October 2016.
6.3.3. The NOP specifies that minimum number of pool tests was three tests per day with the automatic dosing system on and working and every two hours during manual dosing when the automatic dosing system was switched off or not working. The NOP also states that free chlorine levels should be kept at the minimum level– usually between 1.5 and 2.5ppm - to maintain effective disinfection and that free chlorine levels shall not fall below 0.5ppm or rise above 4.0ppm.
6.3.4. Pool management reported that a risk assessment was done on the use of pool dye during a trial session in November 2015, which covered the issues around supervising the pool when it is a different colour, the required disinfection levels, and returning the pool back to normal with appropriate control measures.
6.3.5. The pool dye used was a commercially available product called “Aqua Couleur” from JAK Water systems. The user guide for the product (Appendix 4) specifies that pool water chlorine levels should be maintained below 1ppm and that the colour would dissipate quickly if there was residual chlorine over 1ppm.
6.3.6. Pool management reported that the dye was first used at the launch of the “Big Splash” event at Strood Sports Centre in November 2015 and had been used successfully on at least 10 occasions prior to the 28th Oct 2016 without any incidents or concerns.
6.3.7. It was confirmed that there were no reports of faecal contamination or vomiting episodes at the pool facilities made to the centre staff on 28th Oct 2016.
6.3.8. Pool water records (Appendix 5) showed that the level of free chlorine was 2.09ppm at 0700 hrs on Friday 28th Oct 2016. At 1200hrs, an entry was made in the ‘comments/actions’ section stating “auto off; chlorine coming down” indicating that the automatic dosing system was switched off. The next recorded reading at 1400hrs showed a free chlorine level of 0.24ppm. An entry was made in ‘comments/actions’ section at this time but it was not legible. No further recording of chlorine levels were made after 1400hrs on Friday 28th Oct. The next recorded free chlorine was on Saturday 29th Oct 2016 showing a level of 0.0ppm at 0700 hrs. A corresponding entry was made in the ‘comments/actions’ section stating “DPH dosing up to 2.5ppm’, indicating that a higher level of chlorination was implemented. At 1000hrs, the level of free chlorine was recorded as 2.9ppm.
6.3.9. The leisure manager reported that the automatic dosing system was turned off at 12 noon on 28th Oct 2016 to allow the free chlorine level to drop below 1.0ppm to allow the pool dye to work, however the level should have been maintained above 0.5ppm to maintain effective disinfection. It was reported that the duty manager turned the automatic dosing system back on for at least 1 ½ hours and that free chlorine levels were monitored but these actions and monitored chlorine levels were not recorded on the pool water records. The reasons for non-recording of water test results and actions undertaken are under investigation by the pool management and are not subject of this report. It was reported that due to a failure of Medway Council ICT systems, the till system, credit card machine, telephones, internet or email were unavailable at Splashes on 28th Oct 2016. The leisure manager reported that significant disruption to the operation of the site might partly explain why routine recording of actions and test results might not have been undertaken.
6.3.10. A sample of swimming pool water was taken on 31st Oct 2016 as part of the Centre’s system of routine microbiological testing. The results came back on Thursday 3rd Nov 2016 confirming the absence of standard bacterial pathogens (coliforms, E.coli and Pseudomonas aeruginosa), indicating that the pool water was safe from a bacteriological perspective.
6.3.11. Two out of 9 staff working at Splashes on Friday 28th Oct 2016 reported becoming ill with symptoms of diarrhoeal illness subsequently. Of note, neither of these staff actually went into the pool but would have been lifeguarding the pool and cleaning the toilets & changing rooms throughout their shift.
7. Control measures
7.1. Health advice for cases
7.2. Pool management and disinfection
7.2.1. The leisure manager was informed by a member of the public of sickness linked to the Splashes on the evening of Sunday 30th Oct 2016. An e-mail had been sent to Splashes on Saturday 29th Oct 2016 but this could not be accessed by the leisure manager until Monday morning due to the failure of the council’s ICT system. On being alerted of the illness episode, the leisure manager promptly contacted the weekend duty managers. The leisure manager was informed that the changing rooms had been cleaned as normal on Friday evening and throughout the weekend and that the pool water had been given a high dose of chlorine on the morning of Saturday 29th Oct 2016 following the busy pool party to prepare it for the weekend. The leisure manger was assured that appropriate cleaning and super-chlorination of the pool had mitigated any risks.
7.1.1. Medway Council EHOs and PHE provided infection control and health advice to cases. The school management were advised to inform parents and staff that symptomatic cases should not attend school until free of symptoms for 48 hours.
7.2.2. On Monday 31st Oct 2016, the leisure manager contacted Medway Council’s environmental health team leader to discuss the reported sickness and action undertaken. The leisure manager and environmental health team leader agreed that based on the actions undertaken, the pool was safe to remain open. Nevertheless, as an additional precaution, based on the assumption the outbreak was likely caused by norovirus, it was agreed to conduct a deep clean of the changing rooms and ensure that all hard surfaces were cleaned appropriately. To facilitate this, the pool was closed on Monday 31st Oct 2016 between 1000hrs and 1600hrs.
7.2.3. The leisure manager continued to liaise with the environmental health team leader, who had by this point informed Public Health England.
7.2.4. Medway Council EHOs, pool management and PHE agreed that appropriate cleaning and disinfection had been completed. The pool was reopened to the public at 1600hrs on Monday 31st Oct 2016.
7.3. Communications
7.3.1. PHE and Medway Council communications teams liaised closely in responding to media queries and providing factual updates on the investigations and health advice.
8. Discussion
8.1. Size and impact of the outbreak
8.1.1. Due to the inability to contact all pool users on the affected days, it was not possible to accurately determine the number of people who became ill in this outbreak.
8.1.2. Furthermore, despite our requests for all pool users between 26th and 28th Oct 2016 to complete the electronic survey questionnaire, it is likely that those became ill were more likely to have completed the survey than those who did not become ill. The low response rate to the survey questionnaire would underestimate the overall case numbers, while overestimating the attack rates in the survey respondents stated in this report.
8.1.3. Nevertheless, the outbreak had a moderately high impact in terms of the numbers who became ill, those who sought medical care and missing school or work activities as a consequence of their illness.
8.2. Peak exposure period
8.2.1. Among the 68 cases identified in the epidemiological study, 66 reported entering the pool after 1200hrs on 28th Oct 2016 (when the auto-doser was switched off). Of the other two cases, one reported entering the pool on 28th Oct 2016 at 1100hrs and another entered the pool on 27th Oct 2016 at 1200hrs.
8.2.2. Except for one respondent who visited on 27th Oct 2016, all reported cases attended the pool facility on 28th Oct 2016. PHE, Medway Council and Splashes pool management are unaware of any reports of illness among pool users who attended the pool after 28th Oct 2016.
8.2.3. It must be noted that for practical reasons, we were unable to contact pool users prior to and after the peak exposure period, i.e. those who visited and used the pool before and after 28th Oct 2016.
8.3. Use of colouring dye
8.3.1. There are no published reports of infectious disease outbreaks or adverse health effects linked to the use of colouring dye in swimming pools. To the best of our knowledge, there have been no similar incidents in England in recent years.
8.3.2. As noted previously, the use of colouring dye requires chlorine levels to be reduced to below 1ppm as otherwise the colour would dissipate. To maintain chlorine level above the minimum recommended 0.5ppm but below 1ppm to maintain the colour effect, regular manual checks of chlorine levels and additional chlorine dosing is necessary.
8.3.3. It is likely that any health effects from the use of the dye arise from the temporary reduction of chlorine levels rather than directly due to the dye itself.
8.3.4. Pool management reported using this dye on various occasions previously without any incidents.
8.4. Source of norovirus
8.4.1. Norovirus is commonly transmitted via direct contact with infected persons (person-to-person), consumption of contaminated food and water or contact with contaminated environment.
8.4.2. Given the typical point-source outbreak curve shown in Figure 1, person-to-person transmission is not likely to be the primary cause of transmission in this outbreak. Similarly, acquisition of norovirus through contamination of food is not likely as food was not served to all pool users on 28th Oct 2016, the day of the outbreak. Given the absence of other common exposures in this outbreak, it is likely that cases acquired their infection at the pool facility through contact with pool water, changing rooms, toilets or the surrounding environment or a combination of these.
8.4.3. We were unable to identify the likely source/route of introduction of norovirus in to swimming pool waters and environment. Staff and survey respondents were not aware of any reports of episodes of faecal contamination or vomiting in the pool facility in the days preceding the outbreak.
8.4.4. Noroviruses can be found in faeces in variable numbers even before the onset of symptoms in infected individuals and may be present at low levels in the water environment. The minimum infectious dose for norovirus infection may be as low as 6–10 virus particles, therefore contaminated water poses a significant public health risk (Meschke JS, Sobsery MD, 2001).
8.4.5. Norovirus is the most common pathogen causing gastrointestinal illness in England (Tam et al, 2012). It is known that up to 32% of norovirus infections may be asymptomatic (Graham et al, 1994) and that a gram of faeces from an infected person has approximately 100 billion viral copies (Atmar, et al, 2008). On average, people have about 0.14 grams of faeces on their bodies when they enter a swimming pool (Gerba, 2000). For children, this amount can vary from 0.01 to 10 grams (Rose et al, 1991). Therefore, someone with an asymptomatic norovirus infection can inadvertently contaminate the water in swimming pool and put other pool users at risk. In several published outbreak reports associated with swimming pools, no clear faecal or vomiting incident could be identified, similar to the current outbreak.
8.5. Chlorine levels in water and norovirus
8.5.1. Medway Council’s NOP requires recording of chlorine levels every two hours manually when the auto-doser is switched off. Splashes pool management reported that they intended to maintain free chlorine levels between 0.5ppm and 1ppm as outlined in the NOP. However, pool water records confirmed that free chlorine levels on 28th Oct 2016 were significantly lower than the standard levels routinely achieved at the pool before and after the pool party and on Saturday 29th Oct 2016, the chlorine level was detected as 0.0ppm at 0700hours . Furthermore, there was inadequate recording of chlorine levels and recording of actions undertaken to keep free chlorine levels above 0.5ppm on 28th Oct 2016.
8.5.2. The outbreak primarily affected pool users who attended the pool after 1200hrs on 28th Oct 2016. After the pool water was super-chlorinated on the morning of 29th Oct 2016, the outbreak terminated abruptly. There were no further reports of illness among pool users from 29th Oct 2016 onwards once chlorine levels were restored to standard levels routinely achieved in the pool.
8.5.3. Two staff members and one survey respondent reported becoming unwell but did not enter the pool. There are several potential explanations for this – they did not have norovirus infection, they acquired the infection from other source(s) outside of the pool, they had contact with contaminated water but did not recall it (e.g. drying children with towel) or they may have acquired the infection from contaminated environment (e.g. toilets, changing rooms, etc.) at the pool facility. Unfortunately, it is not possible to conclusively identify the source of infection in these three cases.
8.5.4. It is to be noted that the evidence on chlorine levels in swimming pool waters and transmission of norovirus is limited. A study amongst volunteers suggested that norovirus can survive chlorine concentrations of up to 10ppm, well above the recommended chlorine concentrations in swimming pools (Keswick et al, 1985). However, a cohort study of an outbreak of norovirus associated with a swimming pool in the USA, similarly associated with low pool chlorine levels noted that the outbreak terminated abruptly once the chlorine levels were over 3.5ppm (Podewils et al, 2007). Outbreaks of norovirus in swimming pools are relatively infrequent, suggesting that standard chlorine levels in swimming pool waters may be adequate to limit transmission (Yoder et al, 2004).
8.5.5. Guidance from the Centre for Disease Control and Prevention (CDC) states that 99.9% of noroviruses are inactivated at a chlorine concentration of levels of 1 mg/L with exposure of 4.2 seconds (CDC, 2012). We are not aware of any scientific studies on the effectiveness of lower chlorine levels (0.5-1ppm) against norovirus in pool water.
8.5.6. UK guidance from the Pool Water Treatment Advisory Group (PWTAG) states that free chlorine levels “should be maintained at 1mg/l or below, to an absolute minimum of 0.5mg/l” (PWTAG, 2015).
8.5.7. A review of recreational water-borne outbreaks found that of the seven outbreaks of norovirus resulting from swimming pool exposure, five reports indicated inadequate chlorination and two reports did not contain information regarding disinfection. Inadequate disinfection was defined as absent or insufficient free chlorine (<1 ppm), chlorination or disinfection equipment failure, or inadequate method of disinfection such as improper use of hydrogen peroxide and/or UV light used in swimming pools. The authors concluded that adequate chlorination can be inferred to be an important component in the prevention of norovirus outbreaks originating from swimming pools (Sinclair et al, 2009).
8.5.8. We reviewed PHE records for previous outbreaks of norovirus linked to swimming pools in England and identified one outbreak reported amongst users of a water park in Cambridgeshire in July 2012. In the Cambridgeshire outbreak, water samples from the pool were found to grow coliforms especially at a point after chlorination, suggesting that the pool maintenance and chlorine dosing may not have been adequate. Considering the common use of swimming pools and the relative rarity of norovirus outbreaks linked to pools, it is likely that that standard chlorine levels (i.e.~1ppm) achieved in swimming pools mitigates against the risk of transmission of norovirus.
8.5.9. A possible explanation is that a large contamination incident by an asymptomatic pool user (unreported to pool management) could have introduced a large amount of norovirus particles in the water system. The lower level of free chlorine (below 1ppm) on this particular date may have been inadequate to effectively disinfect the entire body of contaminated pool water.
8.6. Higher attack rates in children
8.6.1. The epidemiological study in this outbreak found that children were disproportionately affected compared to adults.
8.6.2. This finding is line with scientific consensus that children are at higher risk of getting infected in water-borne recreational outbreaks, due to their naïve immune systems and behavioural factors such as poor hand-washing practices, increased likelihood of swallowing water, etc. (Seyfried et al. 1985; Parkin et al. 2002).
8.7. General hygiene measures
8.7.1. Showering before the use of pool is recommended to minimise the risk of biological and chemical contamination of the pool by users (Robinton et al, 1966). Similarly, showering after the use of pool is recommended to remove any body surface contamination by biological and chemical agents in the pool water.
8.7.2. In the cohort study for this outbreak, only 19% and 60% of respondents reported using the shower before and after use of pool, respectively.
8.7.3. The low level of compliance among pool users on shower use suggests little awareness among users of the preventative role of showering in maintaining pool hygiene and in reducing the risk of illness among users.
8.8. Control measures
8.8.1. Following notification of illness linked to the pool, staff and pool management responded promptly and robustly.
8.8.2. Effective actions, in terms of super-chlorination (twice) and deep cleaning of the pool environment mitigated public health risks.
9. Conclusions
9.1. Epidemiological and microbiological evidence confirm that an outbreak of norovirus with a moderately high attack rate occurred among users of the swimming pool facilities at Splashes leisure centre on 28th Oct 2016.
9.2. Prior to this incident, Medway Council had good experience in using the colouring dye by reducing pool chlorine levels below 1ppm without leading to adverse health effects. Environmental evidence obtained following the outbreak at Splashes shows a lack of compliance against Medway Council’s pool operating procedures, particularly on maintaining effective chlorine levels in pool water, recording of routine test results and recording of actions undertaken.
9.3. Epidemiological evidence is consistent with a point source outbreak, although a specific contamination event could not be identified. In other words, it has not been possible to identify how or where norovirus was introduced or spread during the affected period.
9.4. The epidemiological study showed that those who attended the pool after 1200hrs on 28th Oct 2016, submerged their head in pool water or swallowed water had a higher risk of becoming ill compared to those who did not. Furthermore, the outbreak ended abruptly when chlorine levels were returned to standard levels on 29th Oct 2016. This suggests that this outbreak, primarily affecting pool users on 28th Oct 2016, was most likely linked to reduced chlorine levels below 1ppm in pool water on that day.
9.5. A review of scientific evidence shows that chlorine levels of 1ppm or above might be necessary to prevent transmission of norovirus in water. There is a lack of published scientific data to support the current PWTAG recommendation to maintain free chlorine between 0.5 and 1ppm in swimming pool waters.
9.6. Prompt and robust actions undertaken by leisure management and Medway Council environmental team in response to the reported outbreak mitigated further risks to pool users.
10. Recommendations
10.1. Medway Council is advised to investigate the lessons to be learnt in terms of pool management procedures and to implement appropriate remedial actions.
10.2. Medway Council is advised to review the risk assessment for dyeing the pool water. If dyeing of water is deemed as a safe procedure, additional guidance to staff in the swimming pool Normal Operating Procedure document should be provided.
10.3. Medway Council is advised to consider the need for additional training to staff on the need to maintain legible, contemporaneous records of pool water safety including chlorine levels and actions undertaken.
10.4. Medway Council is advised to consider the need for reviewing business continuity plans and any potential impact on pool water safety/monitoring procedures in the event of service disruption due to ICT failure or similar events.
10.5. Medway Council is advised to consider measures to improve the use of shower before and after use of pool by customers.
10.6. Strict compliance with the Medway Council’s swimming pool NOP should minimise the risk of further outbreaks occurring in the future. Enhanced vigilance and oversight should be considered when deviating from normal pool procedures, e.g. when reducing chlorine levels or when auto-doser is switched off.
10.7. Medway Council is advised to share the summary of this outbreak with the manufacturer of the colouring dye and PWTAG to inform their recommendations for future.
10.8. PHE intends to publish the findings of this outbreak in a peer-reviewed journal to inform future research and practice recommendations in maintaining pool water safety.
Acknowledgements
We are very grateful to the members of public for completing the survey questionnaire, without which the analytical study would not have been possible. We would also like to gratefully acknowledge the excellent support received from Medway Council Environmental Health Department, pool management staff at Splashes, Medway Council Communications and Thames View Primary School management in investigating and managing this outbreak.
11. References
Atmar RL, et al. Norwalk virus shedding after experimental human infection. Emerg Infect Dis. 2008 Oct;14(10):1553-7.
Centers for Disease Control and Prevention. Effect of Chlorination on Inactivating Selected Pathogen. 2012. https://www.cdc.gov/safewater/effectiveness-on-pathogens.html
Graham DY, et al. Norwalk virus infection of volunteers: new insights based on improved assays. J Infect Dis. 1994 Jul;170(1):34-43.
Gerba CP. Assessment of enteric pathogen shedding by bathers during recreational activity and its impact on water quality. Quant Microbiol 2000;2:55–68.
Keswick BH, et al. Inactivation of Norwalk virus in drinking water by chlorine. Appl Environ Microbiol. 1985 Aug;50(2):261-4.
Meschke JS, Sobsey MD. In: Britton, G. Human caliciviruses: basic virology, Encyclopedia of environmental microbiology, 2001, vol. 2 New York. John Wiley and Sons. Pg. 1586-98
Parkin, R.T., et al. (2002) Incorporating susceptible subpopulations in microbial risk assessment: pediatric exposures to enteroviruses in river water. J Expo Anal Environ Epidemiol 13, 161–168.
Podewils LJ, et al. Outbreak of norovirus illness associated with a swimming pool. Epidemiol Infect. 2007 Jul;135(5):827-33.
Pool Water Treatment Advisory Group. Code of Practice: The management and treatment of swimming pool water. PWTAG. May 2015 http://pwtag.org/code-of-practice-feb-2015/
Robinton ED, et al. A quantitative and qualitative appraisal of microbial pollution by swimmers: a preliminary report. J Hyg Camb, 64 (1966), pp. 489–498
Rose JB, et al. Microbial quality and persistence of enteric pathogens in greywater from various household sources. Water Res, 25 (1991), pp. 37–42
Seyfried, P.L., et al. A prospective study of swimming related illness. I. Swimming-associated health risk. Am J Public Health 75, 1068–1070.
Sinclair RG, et al. Viruses in recreational water-borne disease outbreaks: a review. J Appl Microbiol. 2009 Dec 1;107(6):1769-80.
Tam CC, et al. Longitudinal study of infectious intestinal disease in the UK (IID2 study): incidence in the community and presenting to general practice. Gut. 2012 Jan;61(1):69
Yoder JS. et al. Surveillance for waterborne-disease outbreaks associated with recreational water – United States, 2001–2002. MMWR Surveillance Summary. 2004;53:1–22